A small introduction to Angioplasty:
Angioplasty is invasive diagnostic and therapeutic procedure. The catheter is passed through peripheral arteries or veins into cardiac chambers and coronary arteries.
Angioplasty is a Greek term that means vessel shaping. The procedure involves widening of clogged arteries (especially coronary arteries- the arteries surrounding the artery like a crown). A tiny balloon is placed on a guide wire, also called balloon catheter and is then inserted into the blocked artery to help widen it. The arteries can get narrowed or blocked primarily due to congenital heart disease; however, there can be other conditions as well.
How Angioplasty is performed?
An angioplasty your doctor can perform to open the blood vessels that supply blood to your heart muscle. These blood vessels are also known as coronary arteries. Doctors often perform this procedure immediately after a heart failure.
The procedure is also called a “percutaneous transluminal coronary angioplasty.” In many cases, they insert a coronary artery stent following angioplasty. The stent helps keep the blood flowing and the artery from narrowing again.
Doctors usually perform this procedure while people are under local anesthesia. First, they’ll make an incision in your arm or groin. They’ll insert a catheter with a tiny inflatable balloon on the end into your artery. Using X-ray, video and special dyes, your doctor guides the catheter up into the blocked coronary artery. Once it’s in position, the balloon is inflated to widen the artery. The fatty deposits, or plaque, get pushed against the wall of the artery. This clears the way for blood flow.
In some cases, the catheter is also equipped with a stainless steel mesh called a stent. The stent is used to hold the blood vessel open and can remain in place after the balloon is deflated and removed. Once the balloon is out, your doctor can also remove the catheter. The procedure may take half an hour to several hours.
Why Angioplasty is performed?
The main purpose of Angioplasty is to widen narrowed arteries; otherwise, there will not be enough flow of blood in the heart, which will, in turn, create a shortage of oxygen. Angioplasty also reduces the risk of heart attack among patients having severely blocked or narrowed arteries. It relieves a person from chest pain that he/she tends to feel when the heart does not get its required supply of blood and oxygen.
What are different types of Angioplasty?
Angioplasty can be divided into four types:-
#1 Balloon Angioplasty
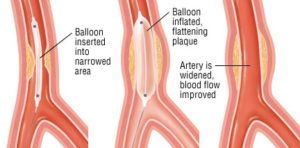
This type of Angioplasty involves the passage of a thin tube, or catheter, into a particular artery through an incision in the upper leg or arm. Then it is directed into the clogged artery. There is a balloon on the tip of the catheter that expands and pushes against the plaque in the wall of the artery to flatten it thereby widening the occluded artery.
#2 Laser Angioplasty:-

The procedures of balloon angioplasty and laser angioplasty are almost similar but in laser angioplasty, the catheter has a laser instead of a balloon on its tip. The laser tip gradually directs to the blocked artery and destroys the plaque layer wise. The laser basically vaporizes the plaque into gaseous particles. It is often used in combination with balloon angioplasty. In such a procedure, first, the balloon attacks the hard plaque and then the laser is applied. Laser angioplasty is not performed by doctors very frequently.
#3 Atherectomy
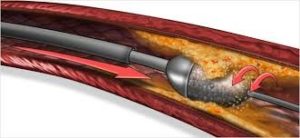
In this procedure, a special instrument is pressed against the fatty deposits of the walls of the arteries instead of a balloon. The instrument basically cuts away the plaque. This procedure is mainly used to treat more calcified (hardened) blockages. The procedure can be divided into various categories:
Extraction Atherectomy : A tiny rotating blade is used in this procedure, which looks similar to a cutter on a food processor. The blade whisks away artery blockages at a rate of up to 1200 revolution per minute.
Rotational Atherectomy: A high-speed diamond-tipped drill is used for this procedure. The drill penetrates into the fatty deposits of the artery wall to remove the blockages and is chiefly used for awfully hard and calcified plaque.
Directional Atherectomy: A special type of instrument is used for this procedure, which is a combination of a balloon and a shaving blade. The shaving blade runs back and forth to shave the deposits on the walls of the arteries away.
#4 Stenting :
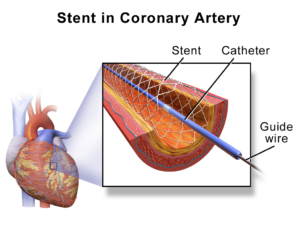
This is a process that is carried out to prevent the artery from closing again. Such a complication is called restenosis. Studies have shown that stents have improved the results of angioplasty greatly. A small metal device in inserted into the occluded artery through a catheter. The procedure is nowadays performed with balloon angioplasty. Direct coronary stenting can also be done but it is not practiced frequently because patients having heart problems often develop blood clots as a result of this procedure.
These are often placed during angioplasty to help keep the coronary artery open. The stent is usually made of metal and is permanent. It can also be made of a material that the body absorbs over time.
Risks of Angioplasty:
All medical procedures come with a certain amount of risk. Just like many other types of invasive procedures, you may have an allergic reaction to the anesthetic, the dye, or some of the materials used in the angioplasty. Some other risks associated with coronary angioplasty include:
- Bleeding, clotting, or bruising at the point of insertion.
- Scar tissue or blood clots forming in the stent.
- An irregular heartbeat or arrhythmia.
- Damage to a blood vessel, heart valve, or artery.
- A heart attack, kidney damage, especially in people who have preexisting kidney problems
- An infection
This procedure is also associated with the risk of stroke, but the risk is low.
The risks of an emergency angioplasty after a heart attack are greater than those of an angioplasty performed under different circumstances.
Feasible Complicatons:
Angioplasty isn’t a cure for blocked arteries. In some cases, arteries can become narrow again. This is called restenosis. The risk of restenosis is higher when your doctor doesn’t use a stent.
Angioplasty is safer than bypass surgery. Less than 1% of people die from complications of angioplasty. Non-fatal serious complications occur in 1% to 5% of people who undergo this procedure. These complications include:
- tearing of the lining of the artery resulting in total blockage and possible heart attack – this can usually is repaired with a stent.
- Stroke from a clot that is dislodged while the catheter is inside the body.
- Bleeding or bruising.
- kidney problems, especially in people with underlying kidney disease and diabetes – this is caused by the iodine contrast dye used for the X-ray; intravenous fluids and medications can be given before and after the procedure to try to reduce this risk.
Which is better for multiple blocks: bypass surgery or angioplasty?
Coronary artery bypass surgery has long been the gold standard for treating artery blockages. Though angioplasty seems to be the winner here due to faster recovery and less incision, CABG is the permanent cure. After CABG, the chance of repeating the procedure becomes very less. Hence, from the point of view of durability CABG is better for multiple blockages.
Angioplasty ensures faster recovery, fewer complications but surgery is the king of the hill when it comes to permanent relief from chest pain caused due to multiple blockages.
Most cardiologists are of the opinion that Surgery is better than Angioplasty for multiple blockages. However, the end decision of treatment lies with the cardiologist and depends on the location of the blockages, your overall health & other factors.
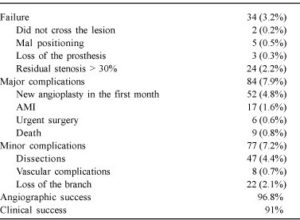
The index of angiographic success was 96.8%, and the index of clinical success was 91%. Angiographic failure occurred in 3.2% of the cases (34 patients), and it was mainly due to residual senses greater than 30% (2.2% of the cases, 24 patients); impossibility of crossing the lesion, mal positioning, and loss of the prosthesis were less frequent (1% of the cases, 10 patients). The most frequent major cardiovascular complication was the need for a new angioplasty (4.8% of the cases, 52 patients), mainly due to acute occlusion (34 patients) or sub acute thrombosis (11 patients). Acute myocardial infarction occurred in 17 patients (1.6% of the cases), urgent surgery in 6 patients (0.6% of the cases), and death in 9 patients (0.8 % of the cases)
.