About Hernia Surgery
Inguinal hernia repair, also known as herniorrhaphy, is the surgical correction of an inguinal hernia. An inguinal hernia is an opening, weakness, or bulge in the lining tissue (peritoneum) of the abdominal wall in the groin area between the abdomen and the thigh. The surgery may be a standard open procedure through an incision large enough
This patient has an indirect inguinal hernia (A). To repair it, the surgeon makes an incision over the area and separates the muscle and tissues to expose the hernia sac (B). The sac is cut open (C), and the contents are replaced into the abdomen (D). The neck of the hernia sac is tied off (E), and the muscles and tissues are sutured (F).
This patient has an indirect inguinal hernia (A). To repair it, the surgeon makes an incision over the area and separates the muscle and tissues to expose the hernia sac (B). The sac is cut open (C), and the contents are replaced into the abdomen (D). The neck of the hernia sac is tied off (E), and the muscles and tissues are sutured (F).
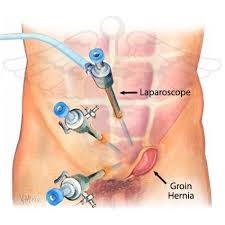
To access the hernia or a laparoscopic procedure performed through tiny incisions, using an instrument with a camera attached (laparoscope) and a video monitor to guide the repair. When the surgery involves reinforcing the weakened area with steel mesh, the repair is called hernioplasty.
Surgery – How it takes place?
For open hernia repair surgery, a single long incision is made in the groin. If the hernia is bulging out of the abdominal wall (a direct hernia), the bulge is pushed back into place. If the hernia is going down the inguinal canal (indirect), the hernia sac is either pushed back or tied off and removed.
The weak spot in the muscle wall-where the hernia bulges through-traditionally has been repaired by sewing the edges of healthy muscle tissue together (herniorrhaphy). This is appropriate for smaller hernias that have been present since birth (indirect hernias) and for healthy tissues, where it is possible to use stitches without adding stress on the tissue. But the surgical approach varies depending on the area of muscle wall to be repaired and the surgeon’s preference.
Mesh patches of synthetic material are now being widely used to repair hernias (hernioplasty). This is especially true for large hernias and for hernias that reoccur. Patches are sewn over the weakened area in the abdominal (belly) wall after the hernia is pushed back into place. The patch decreases the tension on the weakened belly wall, reducing the risk that a hernia will recur.
Risk for developing Hernia
The inguinal ligament is a tight band located between the thigh and the stomach and there are several weak spots along it. Obesity, pregnancy, heavy lifting, chronic coughing, constipation and straining to pass stools can cause the intestine to push against the abdominal wall, and a part of intestine may slip through a weak spot, creating a lump. This lump is called a hernia.
A hernia consists of a sac – the peritoneum – which may contain a piece of intestine (an intestinal loop). It is often able to move inside your body, meaning that it disappears when you lie down, and reappears when you stand up or are straining to pass a stool. The hernia itself is harmless.
However, a hernia can be dangerous if it gets trapped in the weak spot in the abdominal wall and becomes tender. This is known as a strangulated hernia. If the intestinal loop is damaged, its contents can leak out. Gangrene and peritonitis, which can be life-threatening,  may occur as a result. Strangulation is an emergency requiring urgent surgery.
may occur as a result. Strangulation is an emergency requiring urgent surgery.
The hernias can be seen occurring more often among the kids who are known to have one or more of the following risk factors:
What causes an inguinal hernia?
A parent/ sibling who is seen having hernia as a child
- The Cystic Fibrosis
- The Developmental of Dysplasia Over the Hip Area
- Undecided Testes
- The Abnormalities of the Urethra.
A Brief Description
Hernias are divided into two categories: congenital (from birth), also called indirect hernias, and acquired, also called direct hernias. Among the 75% of hernias classified as inguinal hernias, 50% are indirect or congenital hernias, occurring when the inguinal canal entrance fails to close normally before birth. The indirect inguinal hernia pushes down from the abdomen and through the inguinal canal. This condition is found in 2% of all adult males and in 1–2% of male children. Indirect inguinal hernias can occur in women, too, when abdominal pressure pushes folds of genital tissue into the inguinal canal opening. In fact, women will more likely have an indirect inguinal hernia than direct. Direct or acquired inguinal hernias occur when part of the large intestine protrudes through a weakened area of muscles in the groin. The weakening results from a variety of factors encountered in the wear and tear of life.
Inguinal hernias may occur on one side of the groin or both sides at the same or different times, but occur most often on the right side. About 60% of hernias found in children, for example, will be on the right side, about 30% on the left, and 10% on both sides. The muscular weak spots develop because of pressure on the abdominal muscles in the groin area occurring during normal activities such as lifting, coughing, and straining during urination or bowel movements, pregnancy, or excessive weight gain. Internal organs such as the intestines may then push through this weak spot, causing a bulge of tissue. A congenital indirect inguinal hernia may be diagnosed in infancy, childhood, or later in adulthood, influenced by the same causes as direct hernia. There is evidence that a tendency for inguinal hernia may be inherited.
A direct and an indirect inguinal hernia may occur at the same time; this combined hernia is called a pantaloon hernia.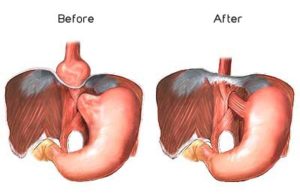
A femoral hernia is another type of hernia that appears in the groin, occurring when abdominal organs and tissue press through the femoral ring (passageway where the major femoral artery and vein extend from the leg into the abdomen) into the upper thigh. About 3% of all hernias are femoral, and 84% of all femoral hernias occur in women. These are not inguinal hernias, but they can sometimes confuse the diagnosis of inguinal hernias because they curve over the inguinal area. They are more often accompanied by intestinal obstruction than inguinal hernias.
Types of Hernia
Indirect inguinal hernias
An indirect inguinal hernia is located in the inguinal canal. In males, this is the location of the spermatic cord.
Typically, the hernia is discovered when it descends into the scrotum.
The hernia may be present at birth.
The treatment for this type of hernia is removal through surgery. Although this can be performed immediately after birth, some surgeons prefer to wait until the child has reached the age of two. Surgery is also the standard treatment for older children and adults.
Direct inguinal hernias
This type of hernia appears later in life.
It is often two-sided. Obesity and hard physical work can contribute to its development. It can be seen and felt towards the middle of the inguinal ligament.
Surgery is again the standard treatment for this type of hernia. Unfortunately, in many cases the hernia recurs and the surgery has to be repeated.
When a very elderly person has a hernia, the doctors may decide not to operate if the hernia is unlikely to cause complications.
Femoral Hernias
Femoral hernias are rare, and mostly seen in middle-aged and elderly obese women who have given birth several times.
The hernia is seen as a lump below the inguinal ligament.
The treatment is surgery.
Symptoms
Inguinal hernia signs and symptoms include:
- A bulge in the area on either side of your pubic bone, which becomes more
 obvious when you’re upright, especially if you cough or strain
obvious when you’re upright, especially if you cough or strain - A burning or aching sensation at the bulge
- Pain or discomfort in your groin, especially when bending over, coughing or lifting
- A heavy or dragging sensation in your groin
- Weakness or pressure in your groin
- Occasionally, pain and swelling around the testicles when the protruding intestine descends into the scrotum
You should be able to gently push the hernia back into your abdomen when you’re lying down. If not, applying an ice pack to the area may reduce the swelling enough so that the hernia slides in easily. Lying with your pelvis higher than your head also may help.
After Care
The hernia repair site must be kept clean and any sign of swelling or redness reported to the surgeon. Patients should also report a fever, and men should report any pain or swelling of the testicles. The surgeon may remove the outer sutures in a follow-up visit about a week after surgery. Activities may be limited to non-strenuous movement for up to two weeks, depending on the type of surgery performed and whether or not the surgery is the first hernia repair. To allow proper healing of muscle tissue, hernia repair patients should avoid heavy lifting for six to eight weeks after surgery. The postoperative activities of patients undergoing repeat procedures may be even more restricted.
Prevention of indirect hernias, which are congenital, is not possible. However, preventing direct hernias and reducing the risk of recurrence of direct and indirect hernias can be accomplished by:
- maintaining body weight suitable for age and height
- strengthening abdominal muscles through regular exercise
- reducing abdominal pressure by avoiding constipation and the build-up of excess body fluids, achieved by adopting a high-fibre, low-salt diet
- Lifting heavy objects in a safe, low-stress way, using arm and leg muscles.
Complications
Complications of an inguinal hernia include:
- Pressure on surrounding tissues. Most inguinal hernias enlarge over time if not repaired surgically. In men, large hernias can extend into the scrotum, causing pain and swelling.
- Incarcerated hernia. If the contents of the hernia become trapped in the weak point in the abdominal wall, it can obstruct the bowel, leading to severe pain, nausea, vomiting, and the inability to have a bowel movement or pass gas.
- An incarcerated hernia can cut off blood flow to part of your intestine. Strangulation can lead to the death of the affected bowel tissue. A strangulated hernia is life-threatening and requires immediate surgery.
Results
Inguinal hernia repair is usually effective, depending on the size of the hernia, how much time has gone by between its first appearance and the corrective surgery, and the underlying condition of the patient. Most first-time hernia repair procedures will be one-day surgeries, in which the patient will go home the same day or in 24 hours. Only the most challenging cases will require an overnight stay. Recovery times will vary, depending on the type of surgery performed. Patients undergoing open surgery will experience little discomfort and will resume normal activities within one to two weeks. Laparoscopy patients will be able to enjoy normal activities within one or two days, returning to a normal work routine and lifestyle within four to seven days, with the exception of heavy lifting and contact sports.
Infection
Swelling over the incision is common after hernia surgery. It doesn’t mean that the surgery was unsuccessful. To reduce swelling and pain, put ice or a cold pack on the area for 10 to 20 minutes at a time. Do this every 1 to 2 hours. Put a thin cloth between the ice and your skin. Call your doctor if you have any of these symptoms:
The incision is noticeably warm and red.
- A testicle is hard and swollen.
- Your wound is bleeding through your bandage.
- You have a fever.
How Well It Works
Open surgery for inguinal hernia repair is safe. The recurrence rate (hernias that require two or more repairs) is low when open hernia repair is done by experienced surgeons using mesh patches. Synthetic patches are now widely used for hernia repair in both open and laparoscopic surgery.
The chance of a hernia coming back after open surgery ranges from 1 to 10 out of every 100 open surgeries done.